-
Large-Volume Intramuscular Injections
INTRAMUSCULAR INJECTIONS
The dorsogluteal site for IM injections is the one nurses have the most experience using, as this is what is traditionally taught in nursing schools and covered in nursing textbooks.16-18 A recent study found that acute care nurses in Canada preferentially selected the dorsogluteal IM injection site over the ventrogluteal IM injection site.19 The majority of respondents cited their own level of comfort as the predominant reason for this preference. However, nurses who were older than 30 years, were diploma prepared, and had more than 4 years of nursing experience were more likely to choose the dorsogluteal site; whereas nurses who were age 20 to 24 years, were degree prepared, and had 1 to 4 years of nursing experience were more like to choose the ventrogluteal site.19 This finding supports the idea that the ventrogluteal site may be used more often by those who received specific guidance in administering at that site.

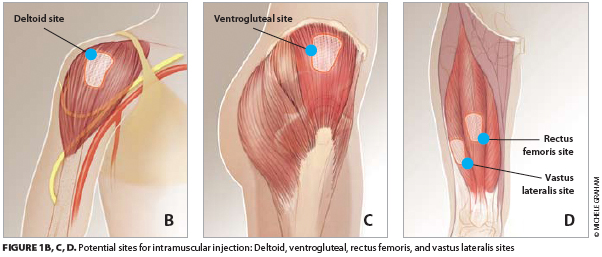
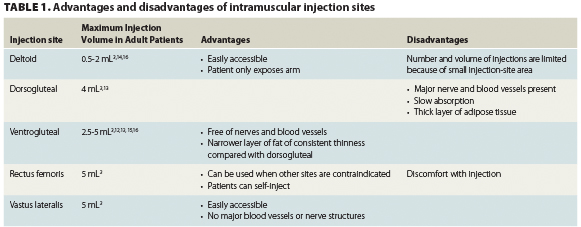
The ventrogluteal region (targeting the gluteus medius1,16) and the vastus lateralis region are free of major nerves and blood vessels.3,17,18 The safety of the ventrogluteal region as an area for administering IM injections is established and the area is identified as a preferred site within clinical practice guidelines.1,3,12,16-18,20 Nevertheless, nurses are reluctant to use this site, possibly because of a lack of confidence in identifying the area or the absence of recommendations by nursing authors or within nursing education.17,18,20,21 The ventrogluteal site is identifiable by a prominent and easily palpable bony landmark; however, it is a small area, which may be an issue in the setting of repeated injections.17,18
Inexperience with injection techniques and inaccurate landmarking can result in injection-site pain or injury.18,22 Sciatic nerve pain can occur, though rarely, if a dorsogluteal injection is given too low.20,23-25 This risk can be attenuated by selecting the upper and outer quadrant of the buttock.3,10 Both the sciatic nerve and the superior gluteal artery are only a few centimeters from this site so care should be taken to landmark the injection accurately.22 Other injection-related side effects are granuloma; intravascular injection; muscle fibrosis and contracture; tissue necrosis; hematoma; abscess; cellulitis; and injury to blood vessels, bone, and peripheral nerves.3,18
ADMINISTRATION BEST PRACTICES
The Z-track method, historically applied to IM injections of irritating medications, can be used for all IM injections to reduce pain and prevent dispersion of medication into subcutaneous tissue1,3,13 (Figure 2). Other strategies for minimizing injection-site reactions are to alternate injection sites and to apply warm or cold compresses to the injection site.29

IN SUMMARY
Evidence-based guidelines for large-volume IM injections will also depend on rigorous research. One area for future research is to determine the optimal amount of time needed to administer large-volume injections, as medications in viscous solutions may take longer to inject. Optimal practices for patients of different weights and sizes should also be investigated because IM injections may be more difficult to administer in heavier patients and older patients may have low muscle mass or integrity. The potential benefits of alternating injection sites, such as between the ventrogluteal and dorsogluteal sites, in order to lessen patient discomfort should be examined as well. Finally, future studies should assess the validity of clinical observations. For example, in our practice, we noted that occasionally patients have discomfort upon sitting after a dorsogluteal IM injection. Two nurses administering fulvestrant simultaneously (ie, one nurse per injection per buttock) has been helpful for patient comfort in our experience. Finally, we found that massaging the area during and after an IM injection helps to prevent and relieve pain.
-
Post Thanks / Like - 11 Thanks, 15 Likes, 0 Dislikes
 PAiN
PAiN,
matrixlifta,
Freedom,
cybrsage,
fairdinkydi,
JACKFTYPE,
Mountain-Man,
Kvasir,
Bustamonky,
IamRonburgundy,
Rsw170 thanked for this post
 PAiN
PAiN,
Freedom,
cybrsage,
JACKFTYPE,
Mountain-Man,
SC,
Kvasir,
JohnDoe,
twisted,
Torcha,
IamRonburgundy,
1ManArmy,
SwoleSooner,
O_high _YO,
Gizmo856 liked this post
----


























































 Reply With Quote
Reply With Quote
Bookmarks