-
💊💊"The dangers of ORAL only cycles"💊💊
"The dangers of ORAL only cycles"
There's a NEW concept of running orals only, on for a few days, switch oral to an other, and switch those, in a repeated interval. (based off an old-school protocol of orals only) Let me explain the hazarded and the potentials for failed results and unwanted side effects.
Here you will read some info I have put together 80% of the read, and some other info I have shared, A mix of feedback and input that explains the hazard and do's and don'ts.. After herring about oral only cycles and switching orals up every few day , here's my take in the instance
Let's talk a bout the "theory" orals off an on.. I'll begin with an opening statement by saying it's simply lousy and ineffective with everything that its attempting to be achieved..Oral hormones need to build a concentration in plasma,serum in the blood,this plasma in the blood medium provides information to other cellular groups that assist with enhancing and improving the drugs effectiveness and efficacy..This is why most (short half life drugs) inherent a protocol for its best advantage, there lets interpenetrate the results "steady,positive blood plasma, expressing optimal drug performance"
Now, you're gonna hear mix reviews on this supported with "regurgitated bro-science" all the while with no actual clinical data citing this to be effective. However, I have seen enough evidence that supports AAS having,creating a environment/platform with needs to have a steady on set/supply to remain effective..Each drug here in questions has a different course of action, half-life, plasma blood build-up etc etc, and each one independently and will imitate different metabolites and enzymes as they share different molecular and chemical structures/rational design and unique functionalities..
With this said: Now lets also take into great consideration AR upregulation with the presence of androgens, more AR sites throughout targeting tissue and these medications in the action in which is desired by the used..,There's a vast amount of activity in which a complex interplay between activation and inactivation mechanisms and signaling between cell groups (now think of all the AAS orals in questions, being used,discontinued and reapplied), what People need to remember that hormones are "chemical messengers" that rely on "CONTINUES" messages/instructions to cells that display specific receptors for each hormone and respond to the signaling..Depending on the compounds and the individuals metabolization ratio the hormone can/may make changes directly to a cell, by changing the genes that are activated (now initiating a response, only to stop and cut it short, for what real reason???), or by making changes indirectly to a cell by stimulating other signaling pathways inside a specific cell group that is effected and effect other processes, thus this can "initiate" an intracellular cascade of events, a slew of unwanted side effects and so on.. So, the notion to utilize orals for a short duration, discontinue and apply a completely different targeting compound will induce imbalance within the endocrine system, within the internal network and switches that are attempting to find homeostasis which represents the body's love of static systems within the body (regulations/rule and order). This applies for the CNS, muscle, fat, hormones, neurotransmitters and brain secretions, as everything needs to be seen within a narrow range. The body has checks and balances, there are many systems of checks and balances in the body. If one fails, there is usually another one which can pick up the slack, and when one level goes up, so will an other, this is all part of homeostasis, but to initiate a war intrancelluar with misfiring, activation, deactivation, awakenings and canalization will only yield a slew of unwanted side effects.. What's the reasons and target purpose? Gains? These " Anabolic Erudite wannabes" from numerous internet panels fail to make mention of blood work, RBC, and BP related issues, or the mechanisms and nuero activation and secretion desensitization? How about a PCT for such a Frankenstein oral stack? What's the long term goals, sides, and potentials... Smoke and mirrors with nothing but just a "new" designer bro stack supported with no actually finds to support its benefits" Absurd, DANGEROUS, and if anyone considers such protocol from a half wit who gave you a piece of his mind, and you held on to it than I'm sure a demitasse would fit his head like a sombrero. And if anyone believes what these crafty entrepreneurs with their million dollar ideas by promoting innovative concepts that seem attractive, but yet possess no clinical data to support short and long term benefits are effective, you might as well stand side by side with them farting peas at the moon!
End result:
Continuous intake of AAS or any therapeutic drugs involves measuring drug concentrations in plasma, serum or blood that will achieve desired effects This information is real life clinical supported text book findings, in which is used to individualist dosage so that drug concentrations can be maintained within a target range, while being fully optimal with its instructions and designed pathways ways and actions..
Drug concentration can NOT be disrupted, and repeated, expecting same or more pronounced effects and the blood plasma needs to build again and again, yielding more stress on the liver, in lieu of being counter productive attempting to hinder liver toxicity... If bloods are routinely measured post-workout,port meal,pro-sup intake, one will see an extreme increase in liver functions aside from AAS used, but attempting to achieve desired or limited adverse effects from orals may correlate better with plasma or blood concentrations than they do with dose that is steady, rather than sporadic, or irregular intervals, ineffective short intakes,and discontinuation and re-administration. Now for these AAS in questions, the positive concentration measurements are a valuable surrogate of daily drug exposure especially to the Androgen receptors which are almost found throughout cellular groups allover the system, as well as FAT and muscle cell/groups, now in-order to initiate a positive nitrogen balance and satellite cell recruitment as well as steady and stable IFG-1 serums by achieving a steady stable/saturated response on AR's in muscle cells to promote size/growth, these AAS orals need continuous supply to keep the blood serum/medium within at the operative ranges and signaling and the same gives for other cellular cascade effects on other cells and AR's or outside the AR's
There's is simply no therapeutically value for athletes and none can be measured when it concerns the pharmacokinetic of these compounds or these protocol variation, individualizing this unorthodox drug dosage, it's difficult for me or anyone that possess some keen understanding on it's actually potentials are.,this is particularly relevant for drugs with a narrow target range or concentration-dependent pharmacokinetics and makes zero sense. Keep in mind that similarly, the variations and effects that are trying to be achieved here can be achieve over time within an individual and results and occur over time for a range of reasons with these drugs drugs using a "SAFER" continuous PROTOCOL, long as there remains a positive blood serum..If not, the agent will loss all effectiveness each time it's started over!
Therapeutic drug behavior is measuring threw drug serum concentrations, not some fancy innovated concept with no backing..
The consequences are seriously and should be placed in to great question by anyway of interpretation of the result in which this is "founded" and by whom made claims that it may produce desirable results without a slew of problems. This requires vast amount knowledge in pharmacokinetics and not something that has been spouted forum or regurgitated a thousands times over.
There's an abundance of clinical research and peer-reviewed data that strongly supports everything I'm advocated
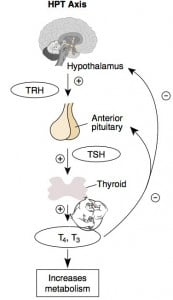
Below is a basic read about the processes taken place with shit down of HTPA
HPTA = Hypothalamic-Pituitary-Testicular Axis
One of the hardest ACTUAL facts to find when searching through steroid and bodybuilding forums is how testosterone supplementation actually shuts you down.
It can be worse than trying to find a needle in a haystack, with a who's who of Bro science "professors" adding their own inaccurate take on things.
So HERE is exactly how Testosterone supplementation (AAS) Shuts you down.
Abbreviations
LH = Luteinizing hormone
HPTA = Hypothalamic-Pituitary-Testicular Axis
FSH = Follicle stimulating hormone
GnRH = Gonadotropin releasing hormone
When exogenous Testosterone any type of steroid derivative is used, a cascade of actions take place in this order.
Your Hypothalamus (This is your master gland in your brain) secretes GnRH, that causes your pituitary gland to secrete LH & FSH.
The increase in these hormones causes the testes to stimulate the Leydig cells to produce testosterone (by conversion of cholesterol). Testosterone then has the ability to undergo various metabolic processes that will inhibit GnRH, which in turn inhibits the secretion of LH and FSH, and that brings a halt to natural testosterone production.
This is referred to as the negative feedback loop. Once testosterone has stopped being produced, it no longer sends this negative signal, and GnRH eventually begins to do its job again.
This is how homeostasis is maintained in the human body.
The whole idea of supplementing with steroids is to override the mechanism for negative feedback.
There is a huge misconception that we can take huge amounts of steroids and we do not have to worry about not producing testosterone because we are replacing it with an exogenous source.
The big problem with this is we have is that certain steroids cause this to a greater degree than others. Estrogenic steroids, or steroids referred to as wet bulking steroids, convert to the hormone estrogen in larger doses, and this causes greater suppression than an androgen alone.
"Aromatization mediates testosterone's short-term feedback restraint of 24-hour endogenously driven and acute exogenous gonadotropin-releasing hormone-stimulated luteinizing hormone and follicle-stimulating hormone secretion in young men" "J Clin Endocrinol Metab. 2001 Jun;86(6):2600-6. The increased estrogen sends signals that there is to much conversion, while your Hypothalamus sends signals that too much estrogen is in your system, so the secretion of LH and FSH is halted. The leydig cells stop producing test, until homeostatis is met, and testosterone has a higher ratio to estrogen than it currently has. Using something to stop this conversion like aromasin, arimidex or letrozole can also decrease the amount of shutdown caused, or speed up the recovery process.
Some steroids are not as inhibitory of testosterone production partly because of the fact they do not confer to estrogen, Anavar being one, and it doesn't saturate androgen recepetors as trenbolone would.
Saturation of the Androgen receptor or increased androgen levels in the blood are the main cause of shutdown, and with steroids like trenbolone, the effects last much longer because the metabolites linger in
CONCLUSION:
Exogenous Testosterone needs to be employed with any oral steroid stack, period!
-
Post Thanks / Like - 4 Thanks, 3 Likes, 0 Dislikes
----
-
Good answer for that all to often asked question.
THANKS
PAIN IS WEAKNESS LEAVING THE BODY
SO DON'T BE A PUSSY
-
Post Thanks / Like - 1 Thanks, 0 Likes, 0 Dislikes
----
-
Very informative brother. I started late in life but I'm in it for the long term I love riding the needle and look forward to saucing way on in my senior yrs.
-
Post Thanks / Like - 1 Thanks, 1 Likes, 0 Dislikes
----
-
Great post, Vision. I can't believe this advice is still floating around. This should be a sticky for those new to designing cycles.
-
Post Thanks / Like - 1 Thanks, 0 Likes, 0 Dislikes
----
-
Good read. Perhaps I'm a little confused by the conclusion "Exogenous Testosterone needs to be employed with any oral steroid stack, period!" as oral steroids are a form of exogenous testosterone. For example, Andriol, is an oral form of Testosterone Undeconate, while Aveed is the injectable form of Testosterone Undeconate. Both injectable and oral steroids are exogenous.
-
Post Thanks / Like - 1 Thanks, 0 Likes, 0 Dislikes
----
-
Good read. The effects of using HCG could be included also.
Sent from my iPhone using Tapatalk
-
Post Thanks / Like - 1 Thanks, 0 Likes, 0 Dislikes
----
-

Originally Posted by
Weapon X

Good read. Perhaps I'm a little confused by the conclusion "Exogenous Testosterone needs to be employed with any oral steroid stack, period!" as oral steroids are a form of exogenous testosterone. For example, Andriol, is an oral form of Testosterone Undeconate, while Aveed is the injectable form of Testosterone Undeconate. Both injectable and oral steroids are exogenous.
Ok, I see your question, and I'll give you the best answer I can..
Just because a hormone is derived from an other doesn't mean it will display the same effects or near, the structures of hormones can be altered.. Example: Bold is derived from Methandrostenolone and it's primary functions and pathways are entirely different.. And Methandrostenolone is derived from Testosterone and yet it's primary functions are different as-well.. So on and so on.. Oral testosterone has been proven to be a piss poor option for treatments..But yes, Andriol is a forum of oral test, known as Testosterone undecanoate, Methyltestosterone is one of the other oral test versions aside from Andriol..But keep in mind that just because other oral hormones are derivatives doesn't mean they will display similar characteristics!
Whether an individual utilized Transdermal testosterone,Testosterone patches, Testosterone gels, creams, and other topical applications,Oral testosterone, Sublingual/buccal testosterone and last but not least -Subcutaneous testosterone pellet they will an extremely difficult time attempting reach the serum levels required to simulate the levels that have been decreased when cycling (HTPA shut down), ..
Clearly I'm talking about oral cycles (Dbol,drol, winny,var etc etc) here as examples, however since you mentioned this oral application you need to take into great consideration and understand that I doubt anyone will be able to afford a Andriol or let alone be-able to obtain it..But, I'll explain the difference with andriol and test in treatments and functions..But, before I do, understand one "MAJOR" disadvantage of orally administered undecanoate is that it is eliminated from the body very quickly, usually in 3-4 hours. Thus, frequent administration is necessary-- usually between 3-6 capsules a day. This can prove to be expensive when compared to injectable testosterone..
Exogenous testosterone can not be duplicated in its 3 courses of action by an other single hormone, below is the functions of test, in which nothing that is synthetically made can duplicate, some may simulate but never duplicate.. Thus, test remains king and the main go-to protocol for TRT, or cycles when endogenous levels are minimal or suppressed entirely..
Testosterone can have 3 roles
1) Being testosterone as it's primary function..
2) Converting into DHT (dihydrotestosterone: a more potent metabolite/androgen)..
3)Converting into estrogen
Here you see this effects differ greatly by individual instances, as genetics, age or even ethnicity (in some cases),or even sex may be a factor, whether one has a greater presence of aromatase enzymes, or even a deficiency..
Hormones/esters have various biosynthetic pathways occurring in the endorcrine,some either or before reaching their target tissue(to control plasma levels or active compounds),
or at times after termination of their actions (inactivation and elimination)..However many of hormones and esters are metabolized within their target tissue,in which a complex interplay between activation and inactivation mechanisms serve to regulate the specificity and the amplitude of the hormonal response..
There's great reason why test is mainly the go-to option that is employed for TRT treatment.. Its courses of action and success ratio and functionality, Andriol isn't used for test replacement for many reasons, effectiveness being one of them, and one can expect to see more effects on their bank account bank account compared to results..
Here is a 3 month study done in Korea, where a pretty small dose of Andriol was administered (160 mg daily for 3 weeks then half that dose for the remainder of the study) resulted in a slight rise in testosterone. Serum total testosterone increased from 2.13 +/- 1.20 ng/ml at baseline to 6.04 +/- 3.08 ng/ml (p = 0.005) after 12 weeks. In addition, free testosterone was (barely) significantly changed from 8.60 +/- 2.25 pg/ml to 11.40 +/- 3.81 pg/ml (p = 0.13) (10).
With this being said: Are you suggesting running Andriol with other orals? To simulate the functionality of testosterone? I would hope not, as this would be a poor option, and it would have been employed long ago if it presented any great value or significant change..
----
-
Brother, I appreciate the time you took to respond to my post. FWIW, I'm already aware of what's written below. Perhaps my post didn't do a good job of conveying what I was intending? So, for dialogues sake, let me try again. Your first post that I replied to went to great length to clarify why an oral steroid cycle is not advisable. Then, in your conclusion, you write the following "Exogenous testosterone needs to be employed with any oral steroid stack, period! I had attempted to suggest that perhaps there may be a better way to word that. I'm assuming (perhaps incorrectly) that you are intending to indicate that injectable testosterone should be employed with any oral steroid stack? Both oral and injectable steroids are synthetic forms of testosterone as you know, and they are both exogenous. So when you say that exogenous testosterone needs to be employed with any oral steroid stack that can perhaps be confusing given that orals are exogenous.
Originally Posted by
Vision
Ok, I see your question, and I'll give you the best answer I can..
Just because a hormone is derived from an other doesn't mean it will display the same effects or near, the structures of hormones can be altered.. Example: Bold is derived from Methandrostenolone and it's primary functions and pathways are entirely different.. And Methandrostenolone is derived from Testosterone and yet it's primary functions are different as-well.. So on and so on.. Oral testosterone has been proven to be a piss poor option for treatments..But yes, Andriol is a forum of oral test, known as Testosterone undecanoate, Methyltestosterone is one of the other oral test versions aside from Andriol..But keep in mind that just because other oral hormones are derivatives doesn't mean they will display similar characteristics!
Whether an individual utilized Transdermal testosterone,Testosterone patches, Testosterone gels, creams, and other topical applications,Oral testosterone, Sublingual/buccal testosterone and last but not least -Subcutaneous testosterone pellet they will an extremely difficult time attempting reach the serum levels required to simulate the levels that have been decreased when cycling (HTPA shut down), ..
Clearly I'm talking about oral cycles (Dbol,drol, winny,var etc etc) here as examples, however since you mentioned this oral application you need to take into great consideration and understand that I doubt anyone will be able to afford a Andriol or let alone be-able to obtain it..But, I'll explain the difference with andriol and test in treatments and functions..But, before I do, understand one "MAJOR" disadvantage of orally administered undecanoate is that it is eliminated from the body very quickly, usually in 3-4 hours. Thus, frequent administration is necessary-- usually between 3-6 capsules a day. This can prove to be expensive when compared to injectable testosterone..
Exogenous testosterone can not be duplicated in its 3 courses of action by an other single hormone, below is the functions of test, in which nothing that is synthetically made can duplicate, some may simulate but never duplicate.. Thus, test remains king and the main go-to protocol for TRT, or cycles when endogenous levels are minimal or suppressed entirely..
Testosterone can have 3 roles
1) Being testosterone as it's primary function..
2) Converting into DHT (dihydrotestosterone: a more potent metabolite/androgen)..
3)Converting into estrogen
Here you see this effects differ greatly by individual instances, as genetics, age or even ethnicity (in some cases),or even sex may be a factor, whether one has a greater presence of aromatase enzymes, or even a deficiency..
Hormones/esters have various biosynthetic pathways occurring in the endorcrine,some either or before reaching their target tissue(to control plasma levels or active compounds),
or at times after termination of their actions (inactivation and elimination)..However many of hormones and esters are metabolized within their target tissue,in which a complex interplay between activation and inactivation mechanisms serve to regulate the specificity and the amplitude of the hormonal response..
There's great reason why test is mainly the go-to option that is employed for TRT treatment.. Its courses of action and success ratio and functionality, Andriol isn't used for test replacement for many reasons, effectiveness being one of them, and one can expect to see more effects on their bank account bank account compared to results..
Here is a 3 month study done in Korea, where a pretty small dose of Andriol was administered (160 mg daily for 3 weeks then half that dose for the remainder of the study) resulted in a slight rise in testosterone. Serum total testosterone increased from 2.13 +/- 1.20 ng/ml at baseline to 6.04 +/- 3.08 ng/ml (p = 0.005) after 12 weeks. In addition, free testosterone was (barely) significantly changed from 8.60 +/- 2.25 pg/ml to 11.40 +/- 3.81 pg/ml (p = 0.13) (10).
With this being said: Are you suggesting running Andriol with other orals? To simulate the functionality of testosterone? I would hope not, as this would be a poor option, and it would have been employed long ago if it presented any great value or significant change..
-
Post Thanks / Like - 1 Thanks, 1 Likes, 0 Dislikes
----
-
Originally Posted by
Weapon X
Brother, I appreciate the time you took to respond to my post. FWIW, I'm already aware of what's written below. Perhaps my post didn't do a good job of conveying what I was intending? So, for dialogues sake, let me try again. Your first post that I replied to went to great length to clarify why an oral steroid cycle is not advisable. Then, in your conclusion, you write the following "Exogenous testosterone needs to be employed with any oral steroid stack, period! I had attempted to suggest that perhaps there may be a better way to word that. I'm assuming (perhaps incorrectly) that you are intending to indicate that injectable testosterone should be employed with any oral steroid stack? Both oral and injectable steroids are synthetic forms of testosterone as you know, and they are both exogenous. So when you say that exogenous testosterone needs to be employed with any oral steroid stack that can perhaps be confusing given that orals are exogenous.
Beside Methyltestosterone/Andriol, oral AAS are NOT synthetic versions of testosterone, they're simply synthetic substances that are "related", .. I think you're missing the principle here my brother.. The most commonly used oral AAS will NOT fulfill the role and characteristic of testosterone, thus the importance to employ synthetic testosterone because of its complex interplay within miltitranscelluar groups and and other internal networks, with activation and deactivation with AR's throught-out the static system, as every hormone has a pathway and destination, some are limited and others are more versatile and multifunctional (i.e. testosterone).. Do you see where I'm getting at here?
----
-
My brother, I'm not missing any principal. What is apparent is that you are misinformed. Both oral and injectable steroids are synthetic compounds that resemble the natural hormone tesotosterone. What is unfortunate is that people who don't know any better may see you as an authority and believe your misinformation. I won't respond beyond this last post as this is just going nowhere. Synthetic Androgens as Designer Supplements
Originally Posted by
Vision
Beside Methyltestosterone/Andriol, oral AAS are NOT synthetic versions of testosterone, they're simply synthetic substances that are "related", .. I think you're missing the principle here my brother.. The most commonly used oral AAS will NOT fulfill the role and characteristic of testosterone, thus the importance to employ synthetic testosterone because of its complex interplay within miltitranscelluar groups and and other internal networks, with activation and deactivation with AR's throught-out the static system, as every hormone has a pathway and destination, some are limited and others are more versatile and multifunctional (i.e. testosterone).. Do you see where I'm getting at here?
----
























































 Reply With Quote
Reply With Quote

Bookmarks